Characteristics of the normal neonatal head CT[2]
- Marked hypodensity of the cerebral white matter,
because of high water content.
In particular,
the frontal white matter exhibits less attenuation when compared to the rest of the white matter in a healthy neonatal brain.
Since most of the brain lesions appear hypodense on CT,
there is going to be a decreased contrast between normal and abnormal tissue when compared with older children and adults.
- Normal differentiation between cerebral and cerebellar white matter and grey matter.
If absent,
gray matter edema should we suspected.
- Marked hyperdensity of the intracranial vascular structures,
because of physiological high hematocrit.
This hyperdensity is sometimes exacerbated because of dehydration.
(Fig.
1)

Fig. 1: Normal neonatal Head CT.
Delivery related: (Fig.
2)
- Skull molding.
- Subdural hematomas: often in asymptomatic newborns,
most commonly located in the posterior fossa.
They may last up to four weeks.
- Extracranial collections (caput succedaneum,
subgaleal haematoma and cephalohaematoma).
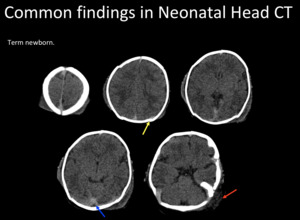
Fig. 2: Common findings in neonatal head. Overlapping sutures (yellow arrow),hyperdense vessels (blue arrow) and subgaleal hematoma (red arrow).
Indications of CT in newborns
CT scan has a pivotal role in the ER,
because of its accuracy to detect bleedings,
fractures and/or mass effect,
with a short acquisition time.
CT scans are often requested to exclude other diagnosis and rule out neurosurgical complications,
in patients with suspected central nervous system infections,
trauma,
non-accidental trauma,
hypoxia and metabolic events.
Hypoxic-ischemic injury
The pattern of injury depends on the stage of brain maturation (gestational age at birth) and severity of the asphyxia.
In case of partial asphyxia,
the perfusion of the most metabolically active areas will be preserved,
but there will be hypoperfusion of the watershed territory (in the new born,
the most metabolically active areas correspond to the myelinated parenchyma).
Radiological patterns of injury:
Prolonged partial injury
- Chronic repetitive stress (for example: nuchal cord)
- Damage of the watershed territory (relatively preserved deep gray matter)
Deep acute injury
- Example: uterine rupture
- Damage of the areas with higher metabolic requirement (basal ganglia,
perirolandic cortex)
Mixed injury
Diffusion weighted imaging (DWI),
is the sequence of choice for the detection of ischemia (cytotoxic edema).
US is also commonly used,
being more reliable for the detection of hemorrhage of the germinal matrix.
There are also well-known CT findings including,
hypodensity of the affected territory,
loss of differentiation between the gray-white matter (secondary to gray matter edema) and mass effect.
(Fig.
3).
The patient may develop a diffuse cerebral edema in deep injuries.
(Fig.
4)
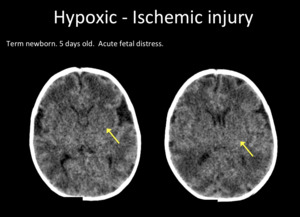
Fig. 3: Axial head CT. Hypodense deep nuclei (yellow arrow), and grey-white matter blurring.

Fig. 4: Diffuse cerebral edema. Axial head CT. Hypodense supratentorial white matter (yellow arrow) and deep nuclei. Blurring of grey-white matter.
Neonatal stroke
Most of the pediatric strokes occur during the neonatal period.
Neonatal stroke encompasses ischemic and hemorrhagic injuries,
in patients older than 20 weeks of gestational age and younger than 28 days of life.
Arterial ischemic stroke (AIS) accounts for 80% of the neonatal strokes,
while cerebral sino-venous thrombosis (CSVT) accounts for 20%.
Ischemic strokes:
The reported neonatal stroke prevalence is 1 case per 1600 to 4000 births (including newborn under 34 weeks of gestational age,
with a reported prevalence of 1 case per 140 preterm births).
AIS may be secondary to thromboembolism or in situ thrombosis (as in older children).
75% of cases are bilateral.
The middle cerebral arteries are the most commonly affected vessels [3].
CT is very useful to distinguish between an ischemic and hemorrhagic stroke.
There are no relevant differences between children and adults regarding CT signs,
including: an hyperdense artery representing an intravascular thrombus-emboli,
blurring of the cortical-subcortical junction,
and basal ganglia and/or cortical hypodensity.
US is also a useful diagnostic tool in the new born,
showing a cuneiform echogenic parenchyma with mass effect.
It is important to remember that US may be normal in the first days after the onset of symptoms.
MRI is the technique of choice to study cytotoxic edema,
especially the DWI sequence,
as already mentioned.
(Fig.
5)
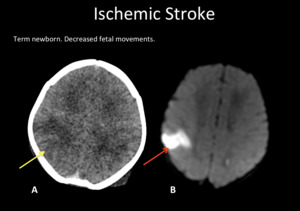
Fig. 5: A) Axial head CT. Right parietal hypodensity with blurring grey-white matter (yellow arrow). B) DWI-MRI shows cytotoxic edema (red arrow).
Hemorrhagic Stroke:
It is defined as intraventricular,
intraparenchymal or subarachnoid hemorrhage.
The reported incidence of symptomatic hemorrhagic strokes in term infants is 0,17 cases per 1000 live births.
[4]
The main risk factors are severe congenital heart disease,
fetal distress,
extracorporeal membrane oxygenation (ECMO),
sepsis and placental abruption.
[4] Other possible etiologies are hemorrhagic transformation in an ischemic stroke,
cerebral venous thrombosis,
choroid plexus hemorrhage,
germinal matrix hemorrhage,
and coagulopathy.
[4] (Fig.
6)

Fig. 6: Left A-V Fistula. A) Transfontanellar US. Coronal plane shows a right occipital hyperechogenic area (yellow arrow). Right intraventricular hemorrhage is recognized. (red arrow). B) Axial head CT, shows a right occipital hematoma with vasogenic edema (yellow arrow), right atrial intraventricular hemorrhage and a left temporo-occipital hypodense area, representing an ischemic lesion adjacent to an A-V fistula (green arrow). C) DWI-MRI shows a left temporo-occipital and insular ischemic lesion.
Venous sinus thrombosis:
Incidence of 0,6 to 12 cases per 100.000 live births [5].
Often multifactorial,
being the most important risk factors: preeclampsia,
maternal diabetes,
perinatal "distress," congenital cardiac disease,
ECMO,
sepsis,
dehydration,
or prothrombotic coagulation defect.
[3]
Locations: [3]
- Superior sagittal sinus: 65%
- Lateral sinus: 50%
- Deep venous system: 50%
- Multiple sites: 50%
The diagnosis of CSVT can be challenging in the new born,
since the intracranial venous structures exhibit spontaneous hyperdensity in non-enhanced CT (Fig.
7).
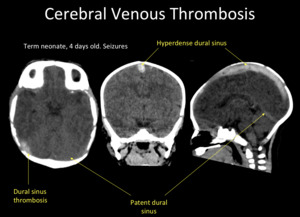
Fig. 7: Unenhanced head CT. Spontaneous hyperdensity of superior sagittal sinus and right transverse sinus in a patient with dural venous sinus thrombosis.
To prevent misdiagnosis,
it is recommended to compare the density of the suspected cerebral vein or sinus with other vascular structures,
for example,
Willis polygon arteries.
Another tool (to avoid the need of CT venography) is the use of Doppler ultrasound,
to prove patency of the sinus.
(Fig.
8)
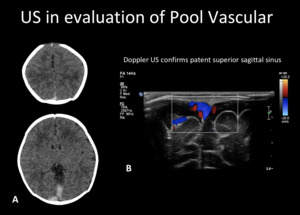
Fig. 8: Evaluation of venous patency with US. A) Axial unenhanced head CT, shows normal spontaneous hyperdensity in the superior sagittal sinus and right transverse sinus, worrisome for thrombosis. B) Doppler US confirms patent superior sagittal sinus.
MRI is the technique of choice to detect the clot using a venography sequence,
and to assess the brain parenchyma status.
Intraventricular hemorrhage
The most common etiology will depend on the gestational age:
Preterm newborn
- Hemorrhage of the germinal matrix
- It can determine hydrocephalus or hemorrhagic periventricular infarct.
Term newborn
- Choroid plexus hemorrhage
- Venous thrombosis


,hyperdense vessels (blue arrow) and subgaleal hematoma (red arrow).")
, and grey-white matter blurring.")
 and deep nuclei. Blurring of grey-white matter.")
 Axial head CT. Right parietal hypodensity with blurring grey-white matter (yellow arrow). B) DWI-MRI shows cytotoxic edema (red arrow).")
 Transfontanellar US. Coronal plane shows a right occipital hyperechogenic area (yellow arrow). Right intraventricular hemorrhage is recognized. (red arrow). B) Axial head CT, shows a right occipital hematoma with vasogenic edema (yellow arrow), right atrial intraventricular hemorrhage and a left temporo-occipital hypodense area, representing an ischemic lesion adjacent to an A-V fistula (green arrow). C) DWI-MRI shows a left temporo-occipital and insular ischemic lesion.")

 Axial unenhanced head CT, shows normal spontaneous hyperdensity in the superior sagittal sinus and right transverse sinus, worrisome for thrombosis. B) Doppler US confirms patent superior sagittal sinus.")